In Part 1 of this blog series, we discussed the fallacy in the arguments used against statins and we briefly explored the vast amount of evidence how statins reduce cardiovascular risk. In part 2 of the blog series, we will continue our journey to explore some latest research on how statins stacked up against other traditional (or no!) therapy in China. We will also look at how "statins causing muscle ache" was recently debunked once more.
How about statin trials in China in recent time?
China has a long distinguished history of traditional medicine for thousands of years - it involves herbal remedy, acupuncture, and the concepts of using certain food substances to restore balance (the "Yin-Yang") in the body. As explained in Part 1, although applying very different principles compared to modern medicine, it is hard to argue that traditional Chinese medicine (TCM) could be very effective in combating many human diseases in ancient China / Asia. However, cardiovascular morbidities and mortalities (heart attack and strokes) were simply not the main drivers of death in ancient societies; and as such, I would argue that we should leave cardiovascular risk reduction to modern medicine and it is in my view unfair to even expect TCM to combat modern cardiovascular disease. Nonetheless, due to geo-political difference in recent time, we are witnessing often an artificial, almost ideological, conflict in the collective mindset, causing deep mistrust of western pharmaceuticals in certain segments of the Chinese population.

Because statins have been so well established for nearly 30 years, it is no longer considered ethical in the Western world to conduct new placebo-controlled randomised trial with statins in patients with cardiovascular diseases. This is because those patients who only take placebo in the control group are inadvertently denied a known effective treatment, hence violating the ethical principles of clinical trial conduct. Recently, however, the research community was surprised to learn of and witness a proliferation of scientific publications from mainland China (often only written in Chinese) that strangely appeared "redundant", i.e. following the clinical guidelines recommending statin treatment published by its very own Chinese Society of Cardiology of the Chinese Medical Association since 2007.
A recent article from John Hopkins University published in BMJ last month found > 2,000 redundant statin trials in China published between 2008-2019 comparing statin to placebo, TCM or no treatment. Worryingly, in the combined 100,000 trial participants in the control groups not treated with a statin, an extra total of nearly 3,500 major adverse cardiovascular events (MACE) were reported, including nearly 600 extra death, > 970 extra heart attacks, > 160 extra strokes, and > 400 extra newly reported heart failure.[3] This is an important meta-analysis for those living in the Western world – even in a country with a long distinguished history of TCM and sophisticated lifestyle modification (or simplification!), statin treatment is clearly shown to be superior for secondary prevention therapy.

Statins and muscle symptoms
As a Cardiologist, the commonest reason I heard patients complaining about statins are muscle pain or myalgia. Statin therapy may cause muscle symptoms (eg, muscle pain or weakness) in up to about 50–100 patients (ie, 0·5–1·0% absolute harm) per 10 000 treated for 5 years.[2] Unfortunately, non-specific muscle symptoms are also extremely common in the general population even without statin treatment. In fact, musculoskeletal complaints are the commonest reason for patients seeking GP consultation and naturally the older age group experiences more musculoskeletal complaints. It is therefore hardly surprising that the age-groups most commonly in need and prescribed statins are also the same groups experiencing the most muscle symptoms.
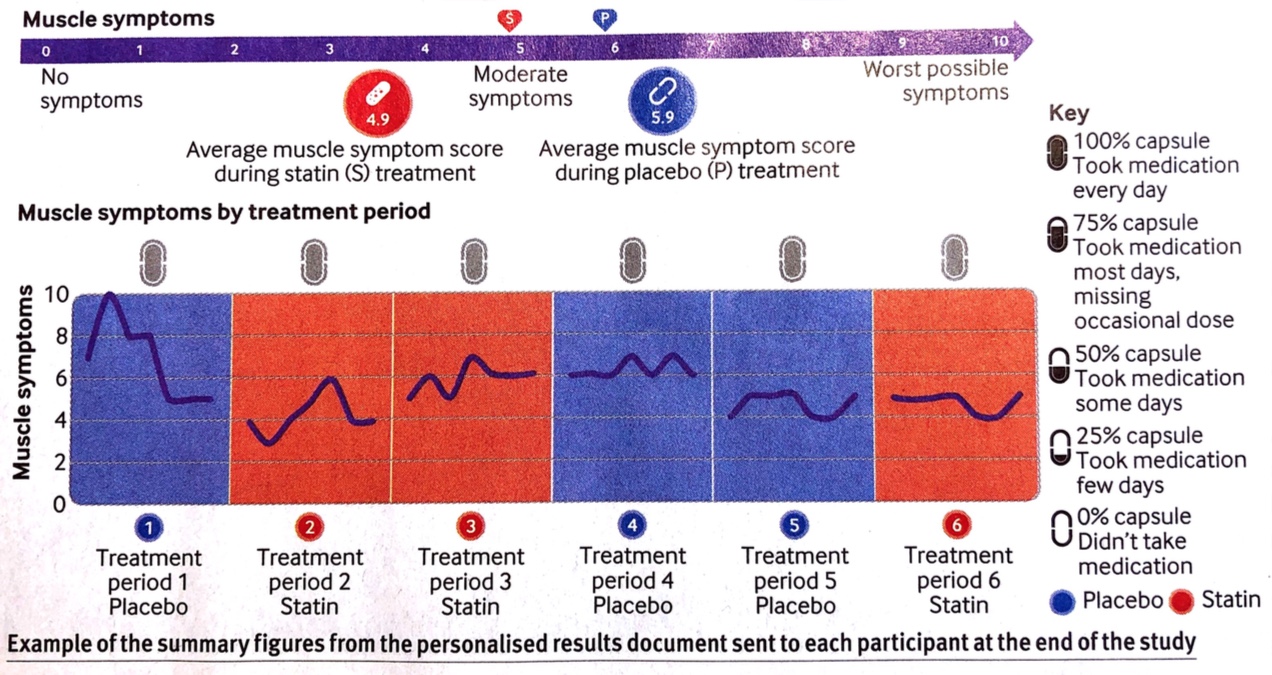
Researchers from the London School of Hygiene and Tropical Medicine reported last month in the BMJ an interesting and carefully-controlled n-of-1 randomised controlled trial series. By n-of-1 trial, each study participant acts as his/her own internal placebo-control. 200 participants who recently discontinued statin therapy were recruited and were randomised to a sequence of six double-blinded treatment periods (2 months each) of Atorvastatin 20mg daily or placebo. At the end of each period, participants rated their muscle symptoms. The overall result of the trial showed that the attribution of muscle side effects was mostly random and there was no overall difference in the frequency or severity of muscle symptoms between to Atorvastatin 20mg versus placebo. Most importantly, most people completing the trial elected to restart taking long-term statin therapy again! [4]
In Part 3 of the blog series, we will continue our journey to discuss how we quantify cardiovascular risk at a population level, and how do we tackle the challenges in applying population statistics in personalised "precision" medicine. Stay tuned :-)
Reference
- The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9
- Collins R, Reith C, Emberson J, Armitage J, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016;388(10059):2532-61 [doi.org/10.1016/S0140-6736(16)31357-5]
- Jia Y, Wen J, Qureshi R, et al. Effect of redundant clinical trials from mainland China evaluating statins in patients with coronary artery disease: cross sectional study. BMJ 2021;372:n48 [doi.org/10.1136/bmj.n48]
- Herrett E, Williamson E, Brack K, et al. Statin treatment and muscle symptoms: series of randomised, placebe controlled n-of-1 trials. BMJ 2021;372:n135 [doi.org/10.1136/bmj.n135]
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2020;41(1):111-88.