From "vulnerable plaque" to "vulnerable patient" - the concept of cardiovascular risk
When someone searches the Internet for statin, he / she is mostly just thinking about the "(LDL)-cholesterol-loweing" action of statins. However, it has been known for more than 20 years that statin in fact does a lot more than just lowering cholesterol level. We now know that statin has immuno-modulating effect to reduce vascular inflammation, it stabilises atherosclerotic "plaque" (the lipid deposits in arteries that ultimately causes heart attack or stroke when ruptured), and it improves endothelial function (the innermost layer of cells lining our arteries), as well as promoting reverse cholesterol transport that could lead to plaque regression, amongst its many other actions. These are collectively known as the pleiotropic effects of statins. This is probably one of the reasons why statin is started on Day 0 immediately after a heart attack to exert its plaque stabilising effect and reduce mortality, even though the cholesterol effect of statin will take a few weeks to be apparent!
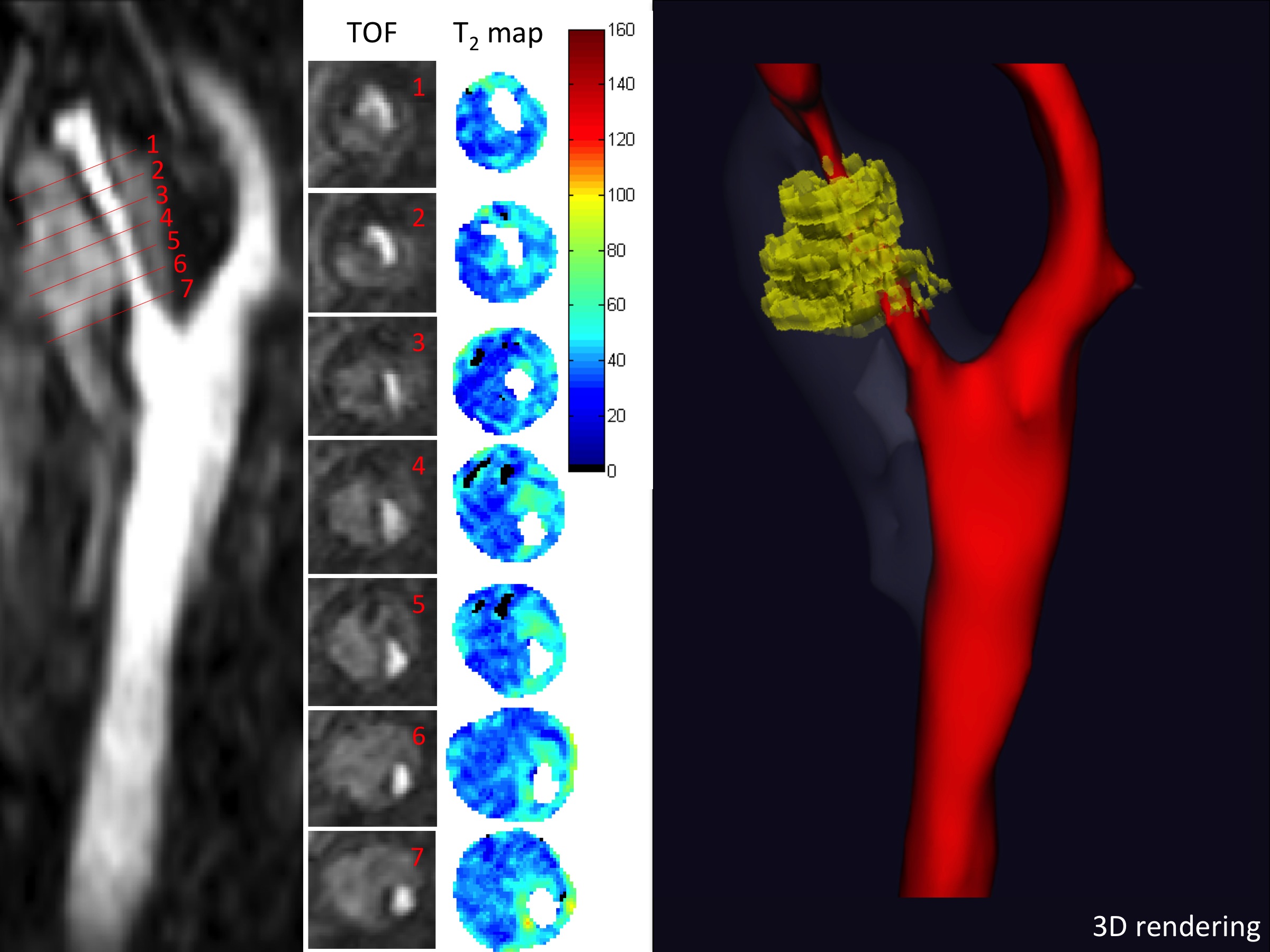
Cardiovascular scientists and cardiologists have been focusing on targeting "vulnerable plaques" for decades - plaques that are cholesterol-rich (with large lipid-rich necrotic core), with thin overlying fibrous cap (thin-cap fibroatheroma, TCFA), that are prone or vulnerable to rupture and then cause acute blockage of the artery resulting in heart attack or stroke. More recently, however, there is an increased awareness that purely focusing on a single / few "vulnerable" plaques are in fact only addressing the "tips" of the cardiovascular (CV) risk iceberg, and there is a gradual paradigm shift to focus from vulnerable plaques to the "vulnerable patient" - which address the total risk of future cardiovascular event. This concept is much especially useful and powerful in patients without prior heart attack or stroke in primary prevention therapy.
Population risk stratification and personalised precision medicine
The absolute benefits of statin therapy ultimately depend on an individual's absolute risk of occlusive cardiovascular events and the absolute reduction in LDL-c that is achieved. In primary prevention, therefore, we often need to risk-stratify an individual’s overall cardiovascular risk using statistical modelling. There are many available statistical tools but the most commonly used risk calculator in the UK primary care is the QRISK3 score (https://qrisk.org/three/), which take into account an individual’s age, sex, ethnic group, and other cardiovascular risk factor such as smoking status, diabetes, family history, BMI, lipid profile, etc. to predict the 10-year risk of cardiovascular events.
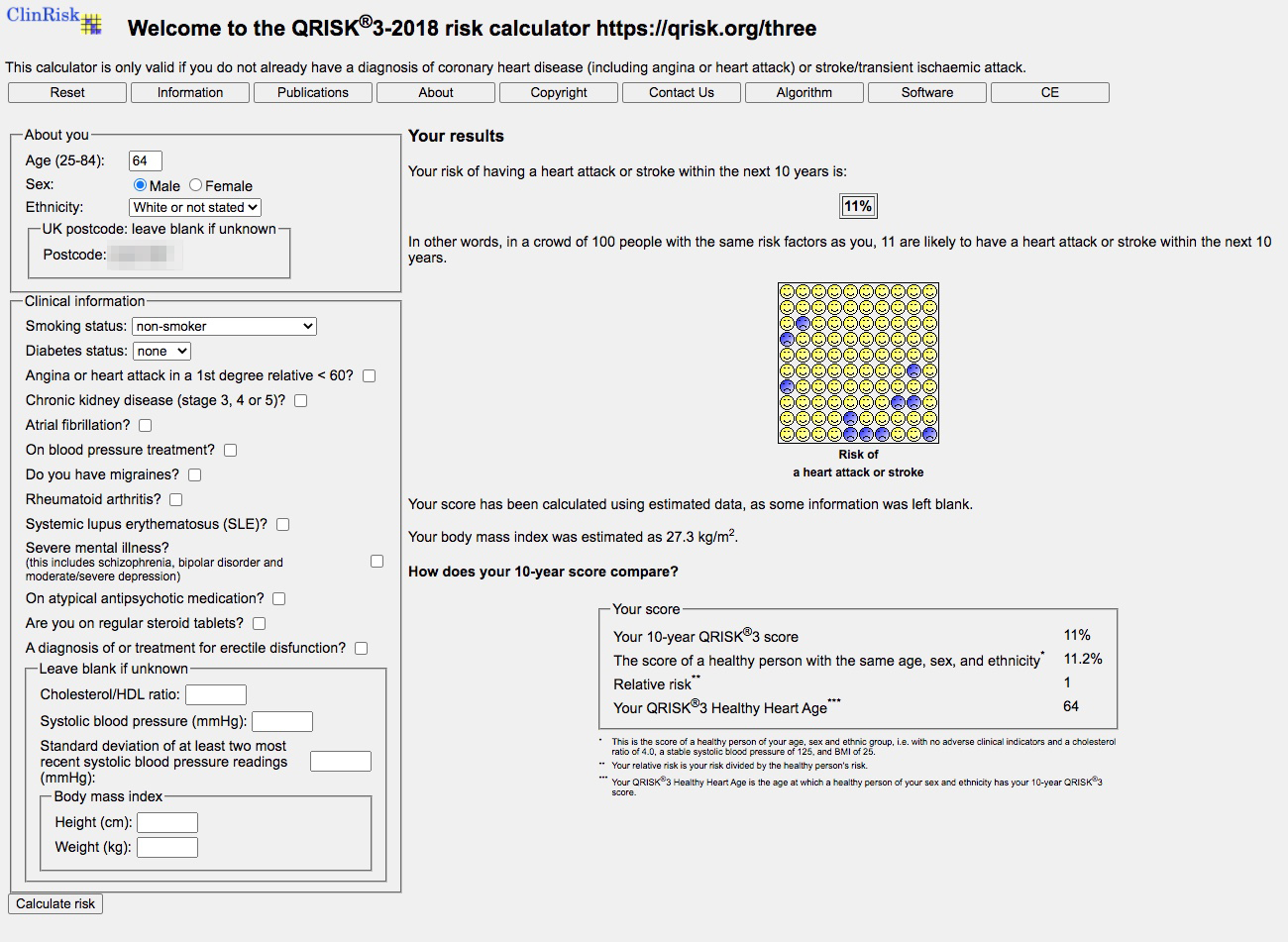
It is very important to remind ourselves that QRISK assessment tool should not be used on people who already have cardiovascular disease such as prior heart attack / stroke / peripheral artery disease or people with known lipid disorder - as these cohorts of patients have already "revealed" themselves to be at high-risk of future cardiovascular events.
People with a 10-year CVD risk of <10% should be offered patient-centred education of cardiovascular risk and lifestyle modification strategy to improve on diet or exercise. Other contributing co-morbidities such as hypertension, diabetes, obesity, should be optimally controlled. Smoking cessation and alcohol reduction advise should always be given. If the 10-year CVD risk is >10%, then in addition to the above non-pharmacological intervention, statin treatment for primary prevention should be considered. Patients with chronic kidney disease will need even more stringent treatment threshold.

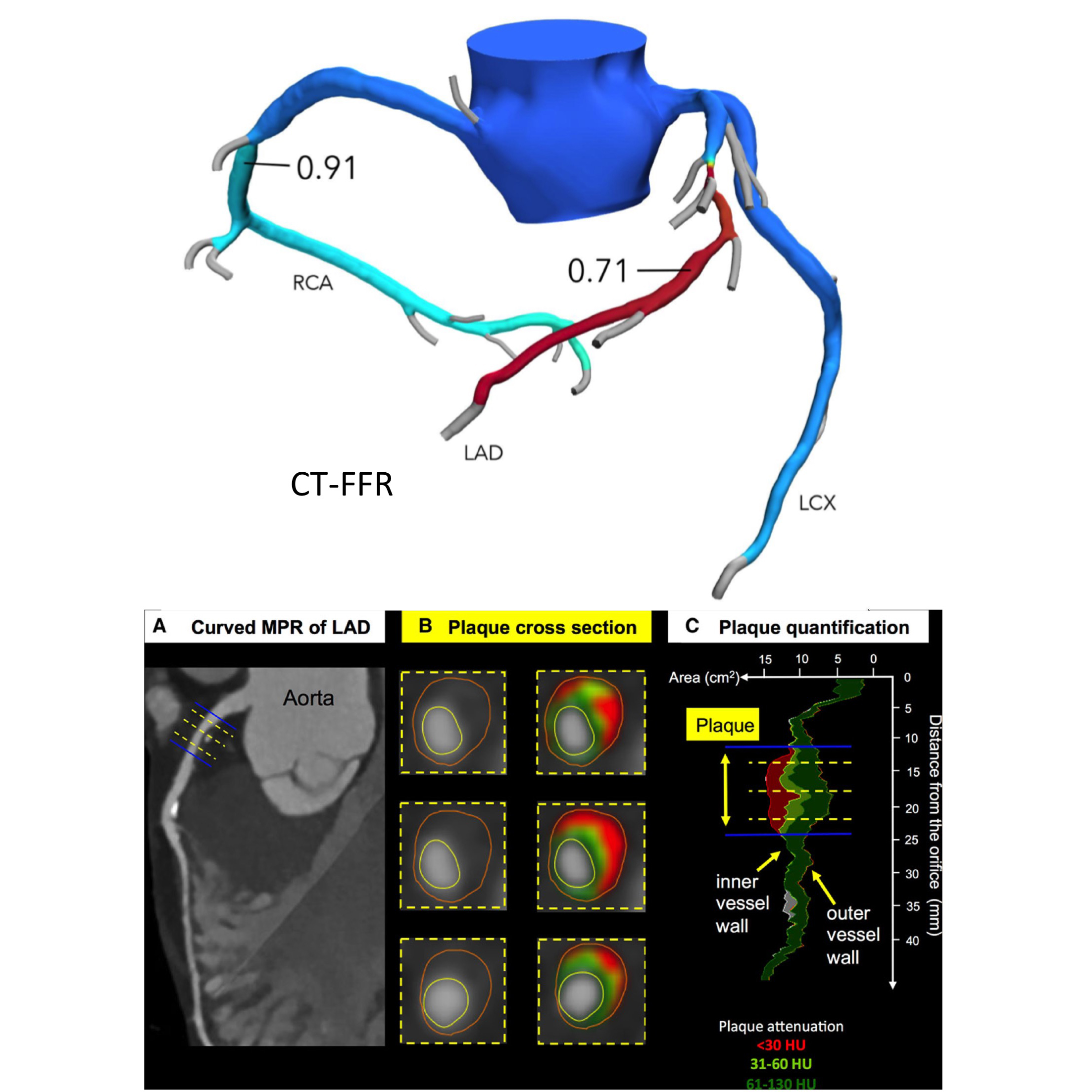
The use of risk calculator like QRISK3 relies on population statistics – and we all know the challenge in applying large-scale population statistics on an individual level. The advance of non-invasive atherosclerotic imaging techniques e.g. Cardiac CT holds crucial promise in individualised risk-stratification towards the ultimate aim of personalised medicine. Applying individualised atherosclerotic imaging in addition to the population-based risk modelling, can increase the sensitivity and specificity of risk prediction and allow tailoring of pharmacological interventions in a layered approach.
At CardioQinetics Heart Clinic, with state-of-the-art research experience in lipid quantification using non-invasive imaging techniques, Dr Chai and his team offer our patients a comprehensive cardiovascular risk assessment and can apply the latest cardiac CT techniques to assess not only for plaque burden, and flow-limitation of coronary lesions, but also compositional analysis to assess for plaque vulnerability. We can then discuss whether standard / more intensive statin therapy is required, or even consider for more advanced biologic therapy to specifically target vulnerable high-risk individuals.
Beyond statins
Recently, the field of lipid / CV risk management is getting exciting again. For a long period of time, we only really have statin and ezetimibe at our disposal. The use of fibrate is limited and nicotinic acid is sadly out of favour after high profile failure of two major cardiovascular outcome trials. The success of PCSK9 inhibitors the FOURIER (Evolocumab) and ODYSSEY (Alirocumab) trials injected new energy in the field. Proprotein convertase subtilisin/kexin type 9 (PCSK9) is an peptide that binds to the low-density lipoprotein (LDL) receptors. If PCSK9 is blocked, more LDL receptors are recycled and present on the cell surface to remove LDL-c from the blood. PCSK9 inhibitors have been shown to further reduce serum cholesterol and cardiovascular risk on statin-optimally treated patients. The National Institute for Health and Care Excellence (NICE) has now recommended the use of PCSK9 inhibitors in patients with high-risk or very high-risk of CV disease if LDL-c targets are not met with statin therapy alone. It also opens a new door for lipid management in patients who are genuinely statin-intolerant. In 2020, yet another new drug Bempedoic acid has come onto the scene and now also been recommended by NICE to treat dyslipidaemia and help combat cardiovascular risk. Therefore, with the powerful reinforced arsenal in fighting cardiovascular disease, cardiovascular physicians and cardiologists worldwide would need to up our games now in educating our patients and dispelling misinformation from irresponsible Internet sources and social media.
Reference
- The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9
- Collins R, Reith C, Emberson J, Armitage J, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016;388(10059):2532-61 [doi.org/10.1016/S0140-6736(16)31357-5]
- Jia Y, Wen J, Qureshi R, et al. Effect of redundant clinical trials from mainland China evaluating statins in patients with coronary artery disease: cross sectional study. BMJ 2021;372:n48 [doi.org/10.1136/bmj.n48]
- Herrett E, Williamson E, Brack K, et al. Statin treatment and muscle symptoms: series of randomised, placebe controlled n-of-1 trials. BMJ 2021;372:n135 [doi.org/10.1136/bmj.n135]
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2020;41(1):111-88.
- Bittner DO, Mayrhofer T, Puchner SB, et al. Coronary computed tomography angiography-specific definitions of high-risk plaque features improve detection of acute coronary syndrome. Circ: Cardiovasc Imaging. 2018;11:e007657