In Part 1 of the CoRe series, we discussed about the evolving concept of complete rehabilitation and how this has rapidly expanded in the field of cancer rehabilitation. In this Part 2 of the series, we will delve into how we can apply CoRe in "prehabilitation" before certain invasive treatment and how we at CardioQinetics are applying this concept to help patients with heart disease.
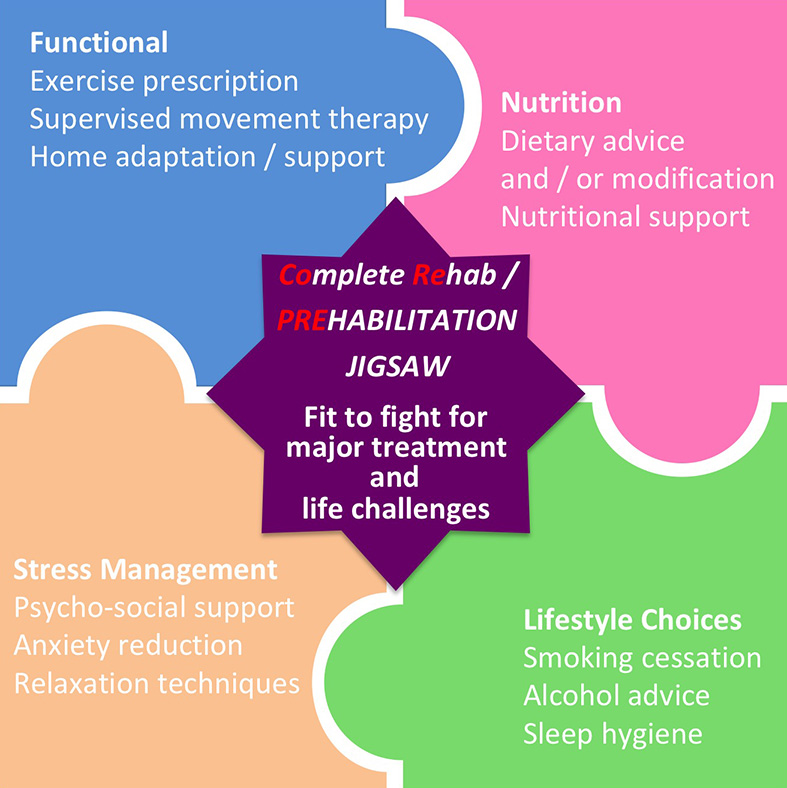
Prehabilitation - "fit to fight" for major treatment & life challenges
The NHS performs over 1.4 million major elective surgery per annum [1], and post-operative complications affect up to 40% of patients after major surgical procedures [2]. This is not to mention the side-effects of many non-surgical treatment modalities such as chemotherapy, radiotherapy, immunotherapy, etc. The risk of surgical complication, as well as susceptibility of unintended treatment side-effects often follow the classic risk profile. Patients who is older, with more comorbidities, perhaps frail with limited mobility and psychosocial support, are naturally more prone to be affected. It cannot be emphasised strongly enough that lifestyle and behavioural factor significantly influenced risk e.g. via physical inactivity, poor general health and fitness, smoking, excessive drinking, suboptimal nutritional status, and adverse psychological factors.
The central concept of pre-habilitation is simple - it aims to enhance general health and well-being prior to major treatment (e.g. surgery), and modify or enhance the "physiological reserve" of the patients by positive physiological and psychological intervention in the peri-operative / post-treatment period, so that to help patients "buffer" the treatment stress response / "weather the storm" of their treatment better. [3]
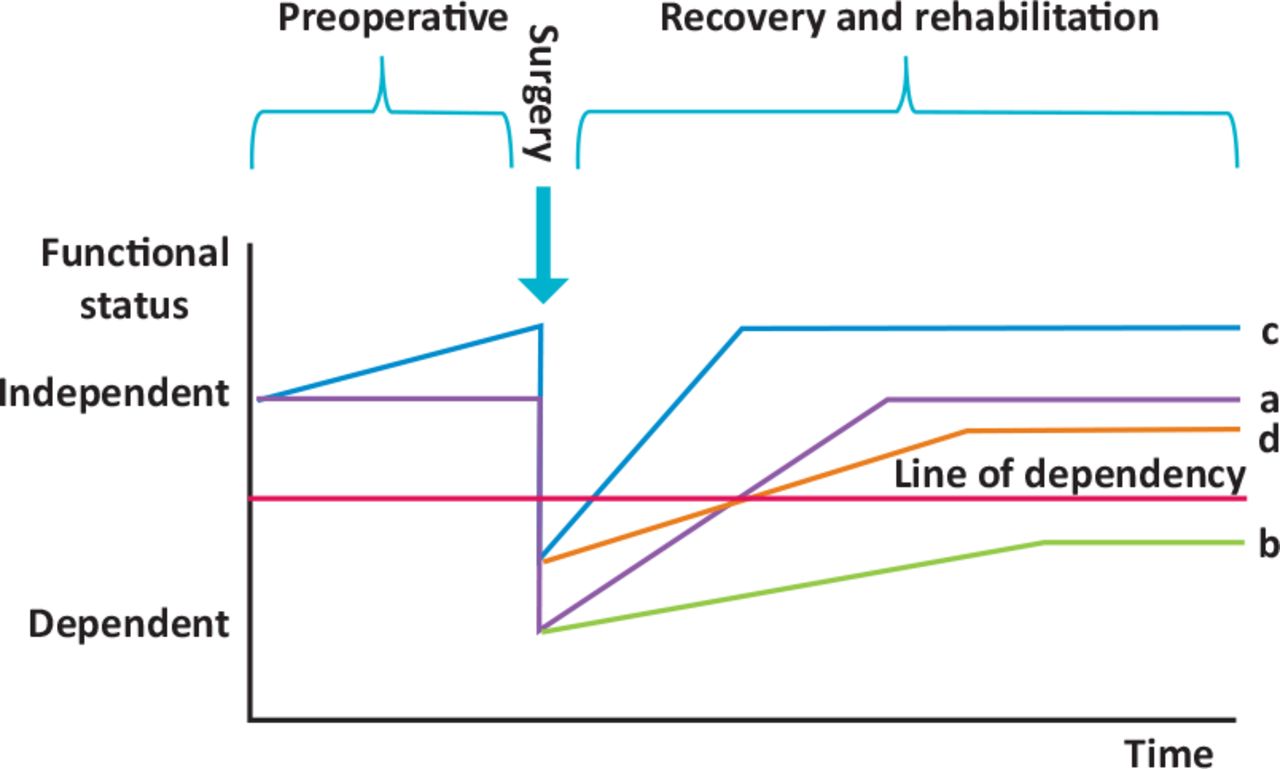
In the above example, Patient A follows a typical treatment journey - with a immediate post-operative functional decline followed by gradual recovery. Patient B suffers a post-operative complication and has a deeper functional decline - as a result despite some functional recovery, he/she may never rise above the "line of dependency". Patient C receives intensive prehabilitation, which raises his/her functional status before the insult of surgery and recovers quickly. Patient D, who also suffers a complication following treatment, is able to bounce back above the dependency line because his/her intensive prehabilitation has raised the baseline [4].
Risk factor prehabilitation
Unhealthy behaviours and lifestyle factors often cluster in the same cohort of patients, and therefore sequential intervention could be too lengthy for the purpose of optimisation before critical surgery. A coordinated multi-modal intervention (see CoRe jigsaw diagram at the top) might offer a more timely and effective intervention programme. Experts now proposed in a "tired" approach to risk-stratify individuals for tailored prehabilitation programme [5].
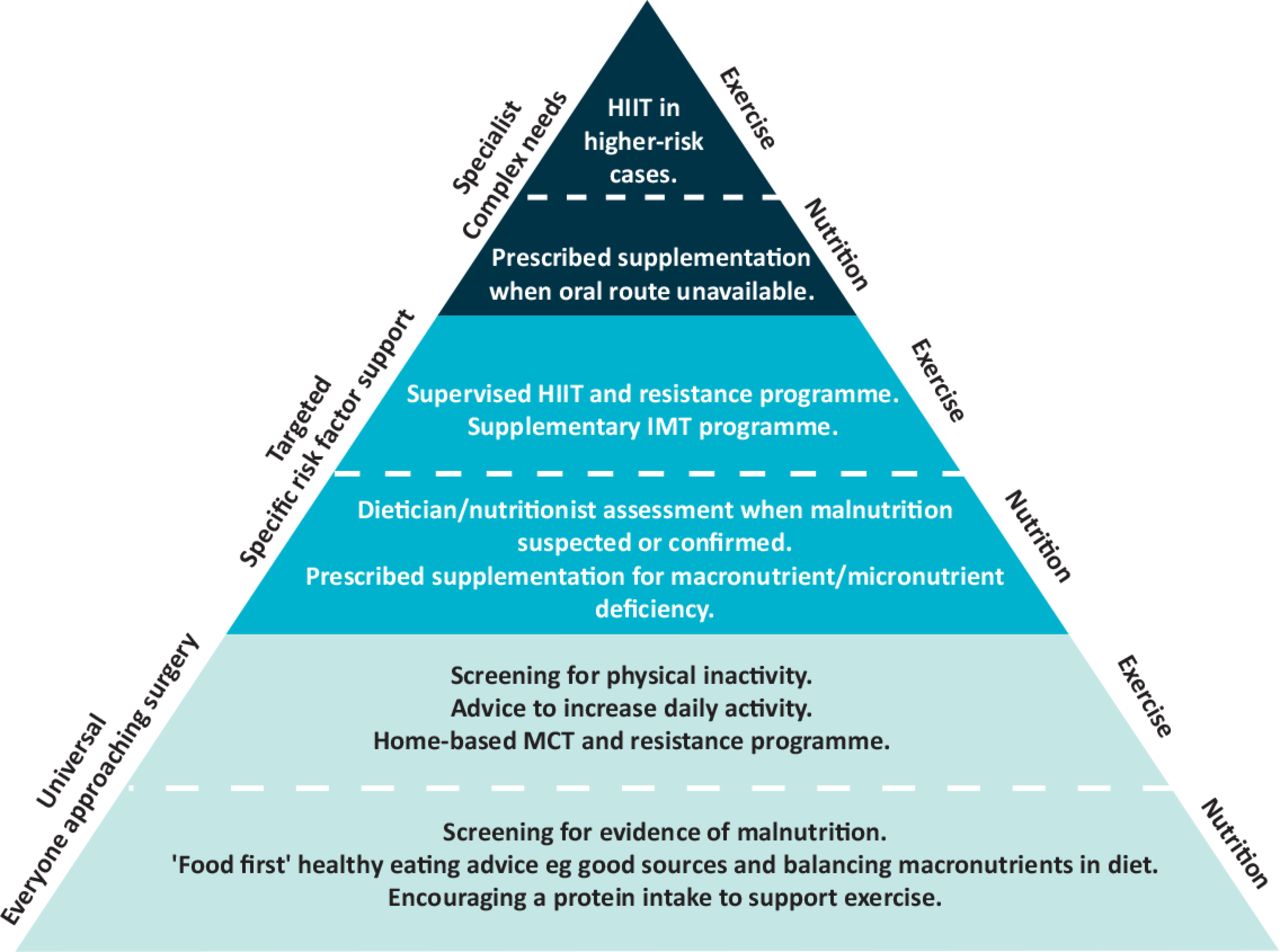
Specific risk factor intervention includes:-
1. Tackling physical inactivity and poor fitness
This is the area where trained physiotherapists and exercise professionals can really provide targeted focussed interventions. Functional capacity as measured by cardiopulmonary exercise test (CPET) is a useful measure for risk stratification. Poor general fitness adversely predicts risk of complications and recovery time following treatment. It also indirectly linked with the psychological wellbeing of patients recovering form often life-changing diagnosis and treatment. Although one-third of the surgical populations may be inactive, physical fitness can be improved within pre-operative timeframes (4-6 weeks) using appropriate exercise programme [6]. Physiotherapists with previous training in respiratory physiotherapy is even more equipped for preoperative inspiratory muscle training to improve overall respiratory function which is often one of the main contributing factors in anaesthetic risks.
2. Nutritional intervention
Pre-operative nutritional support is challenging and often limited by the underlying disease process. Dietician support with nutritional programme and recommendation of diets could play a part to optimise physiological reserve in enhancing pre-operative fitness.
3. Lifestyle modification
Smoking is a major perioperative risk factor affecting the airways in up to 25% of surgical patients. Advice of nicotine replacement therapy and psychological support in smoking cessation can play an important role in improving respiratory reserve and overall fitness. Likewise, Alcohol may exacerbate the neuroendocrine response to surgical stress and reduction in assumption to within recommended level may reduce incidence of post-operative complications.
4. Psychological support
This is an emerging area of prehabilitation practice. The psychological impact of diagnosis, as well as major life-changing surgery, often strips away the patients confidence of independence. Negative mood states, such as depression and anxiety is common in patients undergoing major surgery; and they can adversely affect recovery time and the perceived benefit of treatment. After all, it does not matter if the surgery is a total success, if the patients cannot resume life at a functional level that they feel life is worth living!

Cardiac Rehabilitation
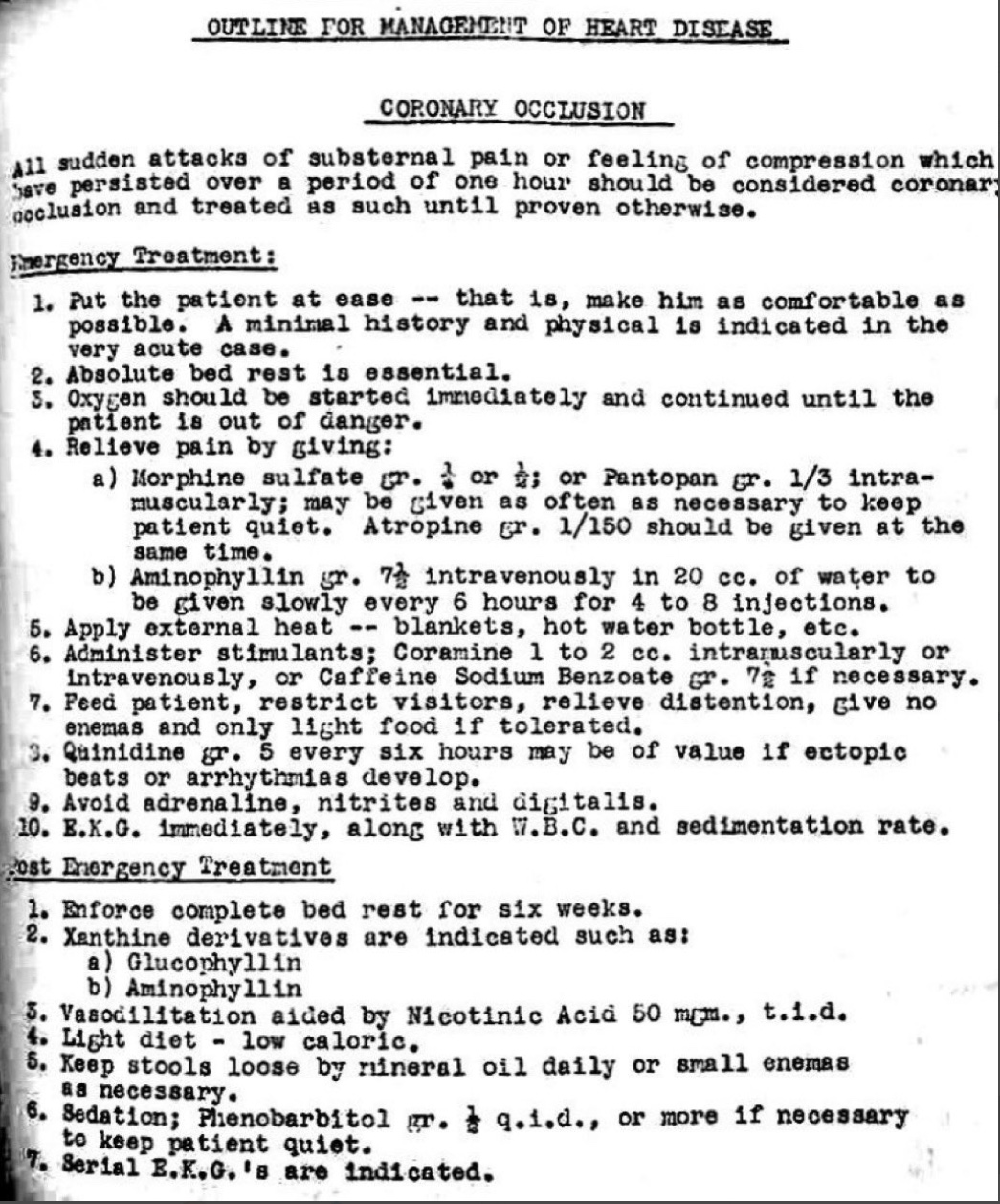
The World Health Organisation (WHO) defined cardiac rehabilitation as "the sum of activity and interventions required to ensure the best possible physical, mental, and social conditions so that patients with chronic or post-acute cardiovascular disease may, by their own efforts, preserve or resume their proper place in society and lead an active life". With its multimodal approach and multidisciplinary involvement, cardiac rehabilitation draws strong parallel to complete rehabilitation described above. Cardiac rehabilitation is now an integral part of the treatment pathway offered to heart disease patients. But it was not that long ago, up until 1940s-50s, that most clinicians in fact believed patients with heart disease should have prolonged bed rest up to 6 weeks - how had we come a long way in the past 75 years!
With the advance of percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG), patients with heart disease now often expect to return to "normal" within weeks of their procedure / surgery. However, what some patients may not appreciate is that successful stenting / bypass is not the end of treatment. It is not even the beginning of the end of treatment, but rather the end of the beginning of a journey of rehabilitation. Using graded exercise and structured education to tackle risk factors and modify behaviour, cardiac rehabilitation has been shown to be very effective in helping patients with heart disease reintegrate back to their normal routine and healthy lives. In fact, cardiac rehabilitation demonstrates cost-effectiveness and significant patient benefits across a range of cardiac conditions in addition to heart attack, e.g. in stable angina, heart failure, or even post-transplant patients. In addition to standard CoRe interventions discussed before, unique to cardiac rehabilitation programme is the opportunity to aggressively tackle blood pressure, diabetic control, and lipid management [7].
A recent systematic review including 148 randomised controlled trials (RCTs) with 98,093 participants concluded that exercise‐based cardiac rehabilitation is an effective and safe therapy to be used in the management of clinically stable people following myocardial infarction or percutaneous coronary intervention or who have heart failure. Psychological‐ and education‐based interventions may also improve health‐related quality of life [8].
Our Cardiac Rehab (CARE) programme - joining force with PhysioQinetics
Dr Chai has a special interest in coronary intervention (stenting and treatment of coronary artery disease / heart attack). He also has a strong research interest in lipid metabolism [9-12]. Dr Chai has combined this with his passion in sports and exercise physiology in directing our sister clinic PhysioQinetics forward for nearly a decade. Recently, CardioQinetics and PhysioQinetics has joined force and are now poised to offer cardiac rehabilitation to our patients - and we call this our "CaRe programme" (CArdiac REhabilitation programme). Dr Chai will be leading this CaRe programme in-house, supported by our team of expert physiotherapists and other allied health professionals. Watch this space - our sister website PhysioQinetics will have more details to follow soon!

Reference
1. Abbott TE, Foelwer AJ, Dobbs TD. et al. Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. Br J Anaesth 2017;119:249-57
2. Hughes MJ, Backney RJ, Lamb PJ. et al. Prehabilitation before major abdominal surgery: a systematic review and meta-analysis. World J Surg 2019;20:1-8
3. Durrand J, Singh SJ, Danjoux G. Prehabilitation. RCP ClinMed 2019;19(6):458-64
4. Tew GA, Ayyash R, Durrand J, et al. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia 2018;73:750-68
5. Macmillan Cancer Support, NIHR Cancer and Nutrition Collaboration, Royal College of Anaesthetists. Prehabilitation for people with cancer: principles and guidance for prehabilitation within the management of and support of people with cancer. Macmillan, 2019.
6. Kothmann E, Batterham AM, Owen SJ et al. Effect of short-term exercise training on aerobic fitness in patients with abdominal aortic aneurysms: a pilot study. Br J Anaesth 2009;103:505-10
7. Mampuya, WM. Cardiac rehabilitation past, present, and future: an overview. Cardiovasc Diagn Ther, 2012 Mar; 2(1): 38–49.
8. Anderson LJ, Taylor RS. Cardiac rehabilitation for people with heart disease: an overview of Cochrane systematic reviews. Int J Cardiol 2014;177:348-61
9. Chai JT, Digby JE, Choudhury. GPR109A and Vascular Inflammation. Curr Atheroscler Rep. 2013;15(5):325
10. Chai JT, Digby JE, Ruparelia N, et al. Nicotinic acid receptor GPR109A is down-regulated in human macrophage-derived foam cells. PLOS One. 2013;8(5):e62934
11. Chai JT, Choudhury RP. Cardiometabolic interventions - focused on transcriptional regulators. Eur J Cardiovasc Med. 2013 Aug 13;2(3):212-18
12. Chai JT, Biasiolli L, Li L. et al. Quantification of lipid-rich core in carotid atherosclerosis using magnetic resonance T2 mapping: relation to clinical presentation. JACC Cardiovasc Imaging. 2017 Jul;10(7):747-56