Physical rehabilitation
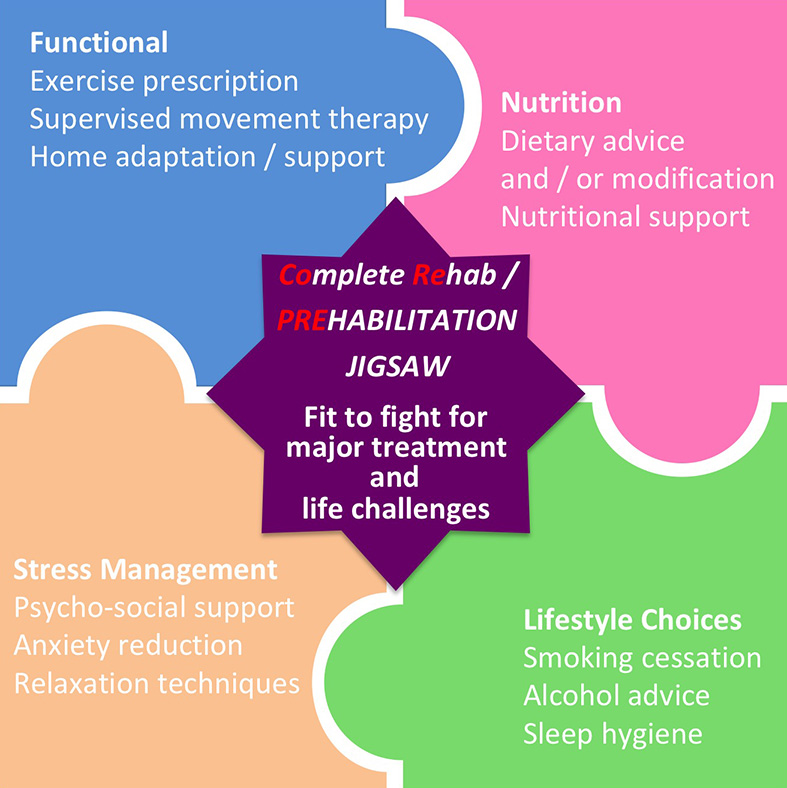
Nearly two and a half centuries ago in 1772 - four years after the very first description of angina pectoris - William Heberden reported the benefit of exercise in the first case of a patient whose angina symptoms peculiarly improved by working in the woods half an hour each day - contrary to the historic belief that one should bedrest to avoid symptoms - more about this later. The therapeutic value of physical therapy (physiotherapy) to improve well-bring and rehabilitation from injury / disease / surgery was quickly recognised; and in 1894, four nurses in Britain formed the Chartered Society of Physiotherapy. Today, physiotherapists-led rehabilitation programmes span across many different fields in medicine:- from high-profile elite sports physical therapy; to the more well-known "bread-and-butter" work in orthopaedic (post-surgery) and neurological (post-stroke) rehabilitation; to the more specialised fields such as cardiopulmonary rehabilitation following heart attack / heart failure / COPDs; and gender / age-specific fields such as women's health and peadiatrics physiotherapy. The "core" concept of physical rehabilitation, however, remains unchanged - to promote physical manipulation, education, and facilitation of graded exercises to improve patients' physical functional outcome. Physiotherapists are therefore uniquely placed to become the central piece in the jigsaw (see diagram above) in coordinating multi-modal rehabilitation programme across different therapeutic fields in complex medical conditions.
Cancer - the archetypal multisystem disease
Not many people recognise the important roles physiotherapists can play with cancer treatment - after all, one might think, what has exercise got to do with chemotherapy / cancer resection surgery? In fact, with the advancement in cancer treatment, more people are living with cancer than ever before. It was estimated that 2.5 million people in the UK were living with cancer (in various stages of diagnosis / treatment / remission) in 2015, and this number is expected to rise to 4 million by 2030. Although most cancers originate as a single-organ disease (e.g. breast cancer, prostate cancer, lung cancer), the totality of consequence of surgery, adjunctive therapy such as chemotherapy and immunotherapy, as well as the possibility of secondary spread, all has major effects on multiple body systems. For example, in addition to recovery from major resection surgery, some cancer treatment has cardiotoxic effect and can impair heart function in certain individuals. Many cancer survivors would suffer tiredness, reduced exertional capacity with muscle wasting, loss of appetite, as well as psychological maladaptation or even depression following diagnosis and treatment. This is a prime example of how a holistic comprehensive rehabilitation programme can benefit cancer survivors.

CoRe - COmplete REhabilitation
Cancer rehabilitation is a good example in the application of the concept of CoRe - COmplete REhabilitation. First introduced in the US, cancer rehabilitation programme has now become an important area of work supported in the UK by charities such as the Macmillan Cancer Support. It focuses on reducing or eliminating side-effects of cancer treatment and improving survivors' strength, as well as their ability to function and to improve survivors' quality of life, through a range of early or even pre-emptive interventions in multiple domains to minimise functional decline. The National Cancer Action Team, working with Macmillan Cancer Support, produced a cancer rehabilitation pathway which details the multidisciplinary approach to intervene at different time-points in the cancer treatment journey, from the diagnosis and care planning, to the actual treatment, to post-treatment care, and even with palliative and end-of-life care.
A successful cancer rehabilitation programme requires the expertise of many different allied health professionals, but many of the specific interventions of common symptoms of cancer (and its treatment), such as anorexia/cachexia/weight loss, breathlessness, continence, fatigue, lymphoedema, mobility issue, and pain, can be carried out or best coordinated by experienced team of physiotherapists.
Some example of specific symptomatic interventions:
(1) Anorexia / cachexia / weight loss
- involving dieticians and nutritionists to design patient-specific dietary regime
- body image adjustment
- assess and address meal time, preparation, kitchen equipment provision
- involving SALT (Speech and Language Therapists) to assess swallowing and how to assist food intake e.g. thickening, etc.
(2) Breathlessness
- assess breathlessness severity using validated tool such as BORG to quantify rate of perceived exertion
- determine factors that exacerbate or ease breathlessness
- pulmonary rehabilitation in breathing exercises and educate self-management for underlying lung condition
- use of respiratory medication such as inhalers / nebulisers / home oxygen
(3) Continence
- assess and improve accessibility to toilet facility
- assess and provide containment products
- provide pelvic exercise advice and programme aimed at muscle strengthening
- discuss medication to help urgency
(4) Fatigue
- involving clinical psychologists to assess fatigue pattern and consideration of cognitive behavioural therapy
- advice on sleep hygiene
- balancing daily activity and regulation of sleep pattern
- Acupuncture and complementary therapies
- environmental adaptation
(5) Lymphodema
- teaching self-management and care of affected limb
- massage therapy and manual lymphatic drainage
- advice on skin care and bandaging
(6) Mobility
- assess equipment to help maintain and improve mobility
- physical exercise programme to strengthen muscles
- assessing and treat specific musculo-skeletal problems
(7) Pain
- work with specialist nurses such as Macmillan nurses to assess and manage chronic pain
- consider massage therapy and acupuncture for pain control
- involving clinical psychologists for cognitive behavioural therapy or even hypnosis

In fact, experts are increasingly aware that in order to maximise the treatment effect and to minimise functional decline, some aspects of the care described above are best delivered before or alongside the actual cancer treatment - a concept now known as "prehabilitation".
On our next episode, we will go into Part 2 of our CoRe series and we will delve further into "Prehabilitation" and why we are energised and poised at PhysioQinetics about exciting new opportunies in apply CoRe / Prehabilitation in other areas of medicine.
Reference
1. Mampuya WM. Cardiac rehabilitation past, present and future: an overview. Cardiovasc Diagn Ther. 2012 Mar;2(1):38-49
2. Cancer in the K 2019. Cancer Research UK. https://www.cancerresearchuk.org/sites/default/files/state_of_the_nation_april_2019.pdf
3. Cancer Rehabilitation Pathways. Macmillan Cancer Support. https://www.macmillan.org.uk/about-us/health-professionals/resources/practical-tools-for-professionals/prehabilitation.html